Chronic Kidney Disease and Racial Disparities in Healthcare
The Barriers
The higher number of Black Americans with kidney failure compared to the lower number of White Americans with kidney failure is a gap or health disparity. A health disparity is the difference in quality of care or health outcomes for a nonminority group compared to a minority group.
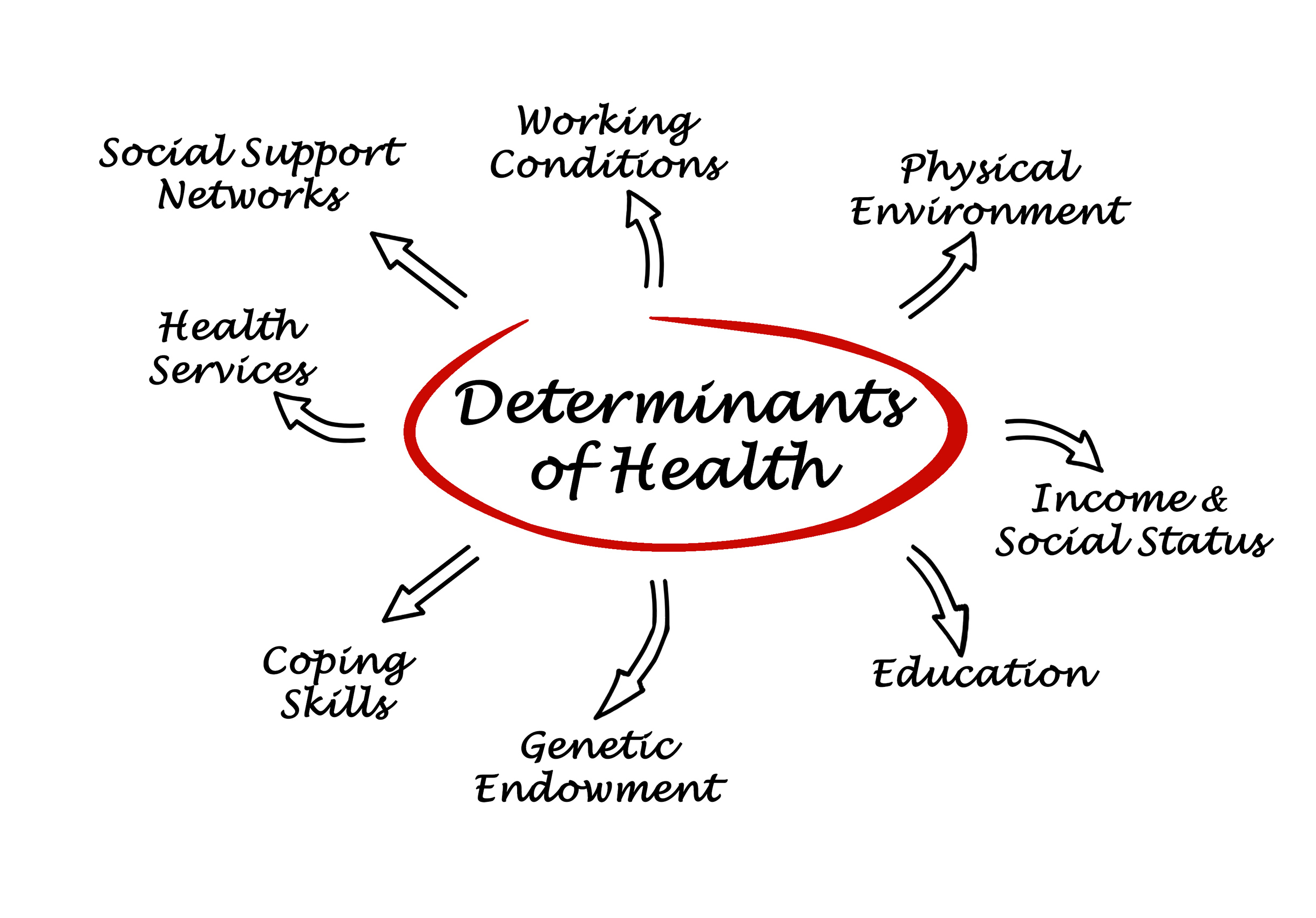
Primary factors that contribute to increased chronic kidney disease (CKD) in Black communities are higher rates of diabetes and high blood pressure. But these are not the only factors. Other barriers are social determinants of health. These include income, employment, education, housing, insurance status, and access to healthcare.
For example, diagnosis and treatment of kidney disease often are delayed for patients in Black communities who have poor access to healthcare. More than 30% of patients with CKD hadn’t seen a nephrologist until the point of kidney failure according to one study. Without timely treatment, CKD can progress more quickly to kidney failure.
Learn more about Social Determinants of Kidney Disease here.
Barriers to Transplant Access
Black Americans with kidney failure have lower access to transplantation. While Black Americans account for 35% of people receiving dialysis, they are less likely to be identified as kidney transplant candidates compared to White Americans. Black patients with kidney disease often encounter barriers throughout the steps to transplant access. They have to wait a year longer on average than white patients to receive a kidney transplant.
Historical Impact of the eGFR Race Correction
In the past, the eGFR race correction multiplier was used in formulas to calculate how well the kidneys were working. In 2021, the National Kidney Foundation and American Society of Nephrology recommended a new approach to eliminate this inequity.
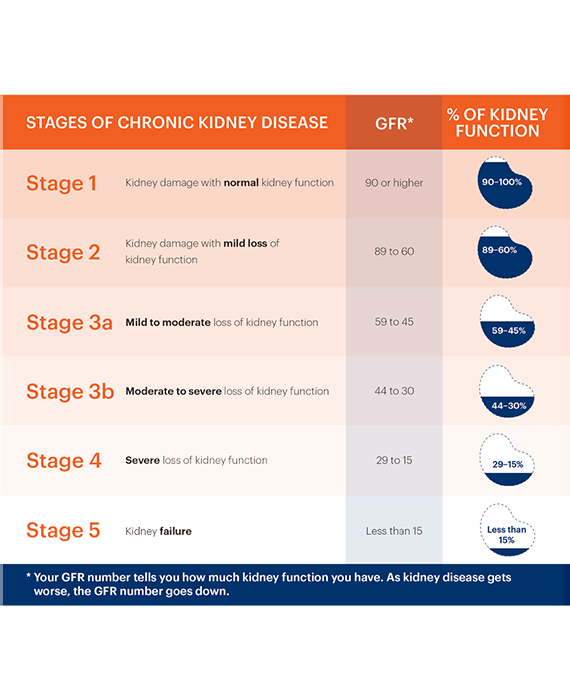
eGFR Calculation
Providers calculate the estimated glomerular filtration rate (eGFR) to determine the severity of a patient’s kidney disease. The eGFR is calculated from the amount of creatinine in the blood using a math equation. Different people can have different creatinine levels in their blood. This difference is not always related to kidney disease. It can be affected by other factors, such as age, sex, and body weight. In the past the eGFR for a Black patient often was multiplied by 1.2 or 1.6, depending upon the formula. However, unlike age, sex, and body weight, race is a social construct. It is not biological. This multiplier prevented Black Americans from getting timely treatment to slow the progression of chronic kidney disease.
eGFR Race Correction as a Barrier to Timely Medical Care
Using race as a factor when calculating eGFR created barriers to timely medical care for Black patients. The multiplier for race can make Black patients seem to have better kidney function than they actually do. When the eGFR race correction multiplier was used, a Black woman who is 5 feet tall and weighs 150 pounds with a creatinine of 2.9 mg/dL and eGFR of >20 ml/min would not be referred for kidney transplantation; a White woman who is 5 feet tall and weighs 150 pounds with a creatinine of 2.9 mg/dL and eGFR of <20 ml/min would be referred. This means that the White patient could get on the transplant waitlist much earlier than the Black patient.
Not only did the eGFR race correction impact access to a kidney transplant, this inequity created other barriers for Black patients with severe CKD:
- Delayed referral to a nephrologist
- Lack of patient education about transplant options
- Inappropriate choice or dosing of medicines
- Potentially harmful levels of contrast dyes used in diagnostic tests
Other pages you may be interested in!

The facts: Prevalence of chronic kidney disease in Black Americans
Know the facts. Compared to other ethnic groups, Black Americans are at increased risk of diabetes, high blood pressure, chronic kidney disease (CKD), and kidney failure.

The biology: Inherited disorders that affect the kidneys
Certain inherited disorders that affect the kidneys are more common in the Black community. These include lupus, polycystic kidney disease, and mutations to the APOL1 gene.