
Patient Candidacy
Prioritize PD for the majority of ESKD patients
At least 78% of patients have no absolute medical or social contraindication for PD1,2
This includes diabetic, elderly & obese patients who are often excluded from PD3-6
Diabetic Patients
Data shows overall patient survival was significantly higher compared with PD than HD in incident dialysis patients with diabetes10
Elderly Patients
Older patients reported significantly better kidney disease-specific quality of life compared to younger patients9
Obese Patients
Single-center retrospective cohort study, obesity also conferred a survival advantage in their PD population compared to non-obese patients7
Younger patients
Among younger patients without and with diabetes in the United States, Canada, and Denmark, PD is associated with survival equivalent to or better than that for HD12
Older patients
In patients with diabetes over 45 years of age, there is no survival benefit for those on HD vs PD, although in the US, HD is associated with better survival12
Modifying factors
Diabetes, age, and comorbidity all significantly modify the effect of treatment modality on patient survival*12
*Data analysis (as-treat and intent to treat) also modifies the effect of treatment modality on patient survival
Regardless of the reported differences in mortality between diabetics on PD and HD, the early initiation of an adequate chronic PD program may ensure higher long-term outcome in PD diabetic patients.11
Passadakis PS, Oreopoulos DG. Diabetic patients on peritoneal dialysis. Semin Dial. 2010;23(2):191-197.

Kaplan–Meier analysis of all-cause mortality according to dialysis modality in the (A) whole cohort of 902 patients and (B) 773 patients who had available HbA1c.
Patients treated with HD showed significantly higher all-cause mortality than those with PD in the whole cohort (log-rank test, P = 0.009) and in 773 patients (log-rank test, P = 0.012). HbA1c = hemoglobin A1c, HD = hemodialysis, PD = peritoneal dialysis.
Adapted from Lee MJ et al. Medicine (Baltimore). 2016; 95(11): e3118.
…the overall patient survival of PD was significantly higher compared with that of HD in incident dialysis patients with diabetes. In addition, better patient survival with PD was influenced by the degree of glycemic control.10
Lee MJ et al. Medicine (Baltimore). 2016; 95(11): e3118
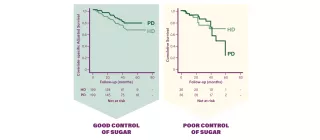
In patients with good glycemic control (HbA1c <8%), the cumulative survival rate was significantly higher in patients on PD than in patients on HD (P=0.021).
However, there was no statistically significant difference in survival in patients with poor glycemic control (HbA1c ≥8%).
- Diabetics with good glycemic control do better on PD than on HD
- Those with poor glycemic control do as well on PD as on HD

Adapted from 2018 USRDS Annual Data Report Reference Tables, Table D.8, Counts of point prevalent ESRD patients, by mode of therapy: peritoneal dialysis
Given the recent outcome data of PD versus HD, older data showing worse outcomes on PD are no longer relevant17,18
Elderly patients with end-stage renal disease are appropriate candidates for peritoneal dialysis
- Most elderly patients possess the manual and cognitive skills necessary to perform PD14
- Elderly patients on PD exhibit excellent compliance with their treatment regimen and display no increase in the rate of infectious complications, though they may have a slight increase in hospital days14. These patients:
- Easily achieve adequacy targets
- Experience good technique survival
- Have nutritional status that is at least as good as that of their hemodialysis counterparts14
- Patient survival varies around the world but is overall comparable to that of age-matched patients on hemodialysis14
- Quality of life may be somewhat superior to that of older hemodialysis patients14
It is not medically justifiable to exclude them from consideration for this therapeutic modality14

Adapted from Griva K, et al. J Adv Nurs. 2014;70(8):1902-1914. *Statistically significant in ANOVA tests. †Statistically significant when analyses were repeated using ANCOVA tests with adjustment for case-mix differences. KDQOL-SF, Kidney Disease Quality
Clinical advice on PD and the elderly patient15
KDIGO in collaboration with the European Renal Best Practice (ERBP) Advisory Board issued clinical advice which states:
KDIGO in collaboration with the European Renal Best Practice (ERBP) Advisory Board
Obese patients should be considered for PD
Overweight and obese peritoneal dialysis patients have longer survival than those with lower BMI – a difference that is not adequately explained by lower transplantation and technique survival rates.7
Snyder JJ, et al. Body size and outcomes on peritoneal dialysis in the United States. Kidney Int. 2003;64(5):1838-1844.
A single-center observational study, obesity also conferred a significant survival advantage in their PD population16
Johnson DW, et al. Is obesity a favorable prognostic factor in peritoneal dialysis patients? Perit Dial Int. 2000;20(6):715-721.

Previous page
Prioritize PD for the majority of patients, regardless of age, race or socio-economic background, by offering equal access to treatment options and patient support services
Next page
Eliminating barriers to PD by addressing health disparities